
Carl Rogers was perhaps one of the most influential psychotherapists of the late 20th century, with his “person-centred psychotherapy” having a lasting impact for many decades later. Attention has recently turned to how psychotherapy achieves its ends in talk, and here Yuanyuan Zhang, from Loughborough University, tells us how – as an aspiring therapist herself, as well as a conversation analyst – she looked into the therapy black box by studying online recordings of Rogers’s own psychotherapy sessions.

My interest in psychotherapy initially started from my role as a psychotherapy client. Later, I wanted to learn the craft of psychotherapy, and this led me to undertake psychotherapy training. I came across Carl Rogers’ recorded sessions during the training course. The trainer played us Rogers’s therapy sessions with “Gloria” and “Dion” (publicly available on YouTube) to illustrate the psychotherapy process and invite students’ comments.
I didn’t pursue the training, but instead became fascinated by what Rogers was doing in his sessions, and I decided to make it the focus of my doctoral work.
Recordings to demystify therapy
Carl Rogers is one of the founders of humanistic psychology and a key figure in psychotherapy. As an initiative to demystify the psychotherapy process, he started recording therapy sessions for research and training in the 1940s. In a catalogue compiled by Lietaer and Brodley (2003), they list 158 session transcripts with 51 clients. The total number of existing recordings (in both audio and video format) is unclear. The primary archive includes, e.g., University of California Santa Barbara Library (see Lietaer and Brodley, 2003, for a comprehensive list).
For my PhD project, I use the recordings already available on YouTube to ensure data accessibility for readers. I collected ten videos in total with the primary search words “Carl Rogers” and “therapy”, in combination with subsequent algorithmic recommendations.

The way I approach the data is to identify the most basic activities in each session as I go through the recordings. Then I compare the activities across sessions with a view to find the commonality. Once I see what routinely occurs, I note it down and put the relevant transcripts together to build the collection. The pattern usually emerges after I go through a few videos. The challenge to work with psychotherapy data is that the clients’ tellings are long – they constitute the bulk of the session. I sometimes get lost because I get overly occupied by the topic (the ‘talked-about’ in Schegloff’s term) and find myself analysing the semantic relationship between sequences of telling. It rarely got me anywhere though. In situation like this, I remind myself “my focus here is the procedure of the therapy, not the topic”.
What’s in the data
What I see from the data is that the main activity for the client is to produce tellings (narrative description of any topic), and for Rogers, it is to formulate the client’s tellings at each completion point. Formulation sustains the ongoingness of the client’s telling, because after marking the receipt of it, the client usually produces more tellings, whether it’s a modification, expanded (dis)agreement, topic shift, and so on. The client’s initial launch of telling does not come from nowhere. It usually relies on Rogers’ elicitation (T = Rogers):

And it is Rogers who routinely initiates the closing of the telling phase, as we see in Extract 2:

What comes before and after the telling phase is the opening and closing of the interaction. In a nutshell, the sequential activities of a Rogerian therapy session are open the interaction, open the tellings, sustain the tellings, close the tellings, and close the interaction.
Keeping it going.
To keep one sequence of telling going, Rogers routinely produces minimal token such as “mm hmm” to mark the receipt while simultaneously treating the telling as incomplete. The completion point of the client’s telling is negotiated. Consider the stretch of talk below. The client (here “Kathy”) has been recounting an experience, and has got to the point (at line 5) where she feels very very (0.4) frightened .hhhhh o:f u:h (.) new male relationships?. Is this the end-point of her account?
See how Rogers, at line 10, offers a formulation of what she has said: so in some way his death .hhh u:hhh .hh (0.3) >really made you< aware of the fear you ha:ve of >new relationships<. That is not quite the same: Rogers has added the insight of her awareness of her fear, and that is now available for her to reflect on.
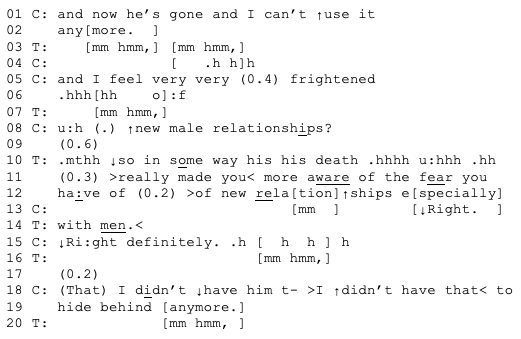
While formulation can serve multiple functions simultaneously, a basic one regarding the interactional structure is topicalising a new insight, and prompting agreement from the client. So Rogers’ minimal token keeps one telling sequence expandable and the formulation keeps the client’s tellings going across sequences.
The structure of Rogerian psychotherapy is unique in that the tellings are kept open and ongoing till the session’s time runs out. Whereas in medical consultation for example, the client’s troubles-talk (a form of telling) closes before the doctor’s diagnosis and treatment recommendation (Robinson, 2003). The troubles-talk between intimate friends does not sustain as long either. Advice, idioms, and positive projection are common practices to exit from friend’s troubles-talk.
What I have learned is that it’s very important to bracket my preconceptions and assumptions and focus on what happens in recordings. Therapy interaction is not easy to work with, particularly this type of historical data. There are too many ideas about what Rogerian therapy is and should be (including Rogers’ own theory!).
Who are these recordings for?
The recordings I obtained for PhD study, genuine as the therapy might be, are cinematic products, meant to demonstrate Rogers’s methods. The Gloria, Kathy, Mr. Lin, Dion, and Sylvia videos each have their own production team. For the Gloria film for example, there is a producer and director (Everett L Shostrom, PhD) and a cinematographer and editor (Rod Yould). There are more caveats. We know little about about the selection and recruitment of clients. Even in terms of the fidelity of the talk, Rogers’ overlaid commentaries in some recordings result in the partial loss of interaction data.
These limitations raise questions about the nature of these recordings: who are they for, does the demonstration count as psychotherapy interaction, and who is to define. These recordings span several decades. The discourses on mental distress and social deviance evolve through time. It takes extra labour to understand the social circumstances of clients from different eras. But the emotional weight of witnessing the client’s pain and unresolved struggles does not disappear when I stop playing the recordings.
Still relevant?
In contemporary psychotherapy, there is an explosion of modalities, such as, art/music/dance/eco therapies, somatic experiencing, etc. The resources, practices and formats that the therapist uses to draw out the client’s personal narratives are certainly more diverse than those of Rogers. However, formulation is still a core practice till this day. The extent to which formulation is used, when it is used, and how it is constructed depends on what interactional activity is going, what the therapeutic task at hand is, and more broadly the therapist’s theoretical orientation.
The contemporary psychotherapy discourse on what therapy is and does is elusive, as it is more result-oriented: it is more focussed on facilitating the client’s emotional and cognitive change, rather than session-based, i.e., focussed on what the client and therapist do from the opening to the closing in the session. Identifying the interactional structure of a Rogerian therapy gives me the clarity as to what psychotherapy is and does.
References
Lietaer, G., & Brodley, B. T. (2003). Carl Rogers in the therapy room: A listing of session transcripts and a survey of publications referring to Rogers’ sessions. Person-Centered and Experiential Psychotherapies, 2(4), 274–291. https://doi.org/10.1080/14779757.2003.9688320
Robinson, J. D. (2003). An interactional structure of medical activities during acute visits and its implications for patients’ participation. Health Communication, 15(1), 27–59. https://doi.org/10. 1207/S15327027HC1501_2
